
When we can’t smell, the sensation is very disturbing. The flavor of food that we detect is 70% related to smell. Smell or olfaction is such an important but often underated human sense. Our sense of smell is one of the most primitive sensory functions in humans. Many thousands of years ago, it was our primary sense to detect food, avoid danger and to find a mate. While in modern life, scavenging for food no longer requires a great smell but google and your e-wallet, the olfactory sense is still linked to the very primitive emotions.
Olfaction drives the valence of the odorous item, whether is be pleasant or not. The sense of smell is associated with food, localization, memory, appetite, detecting spoiled foods and warnings against danger (microbial threats, poisonous fumes). Aromatherapy and phytotherapy (essential oils and fragrance) are often cited to enable pain relief, relaxation, anxiety reduction and enhanced energy.
Although many patients will say they can’t smell, there are several types of olfactory disturbance that can occur. We describe smell loss as Dysosmis (difficulty with odor identification), Paraosmia (sensation of an odor different that the typical for that substance) and Phantosmia (perception of an odor when none is present). Hyposmia is simply the diminished ability to detect odours and Anosmia (the complete lack of smell).
The common causes of smell loss from population studies, are:
- post viral upper respiratory infection (URI) (18–45%)
- nasal/sinus disease (7–56%)
- head trauma (8–20%)
- exposure to toxins/drugs (2–6%)
- congenital anosmia (0–4%)
Assessing for smell loss
We currently perform three component to assess the olfactory system, Firstly we examine the nose and olfactory cleft as part of an overall history and examination:
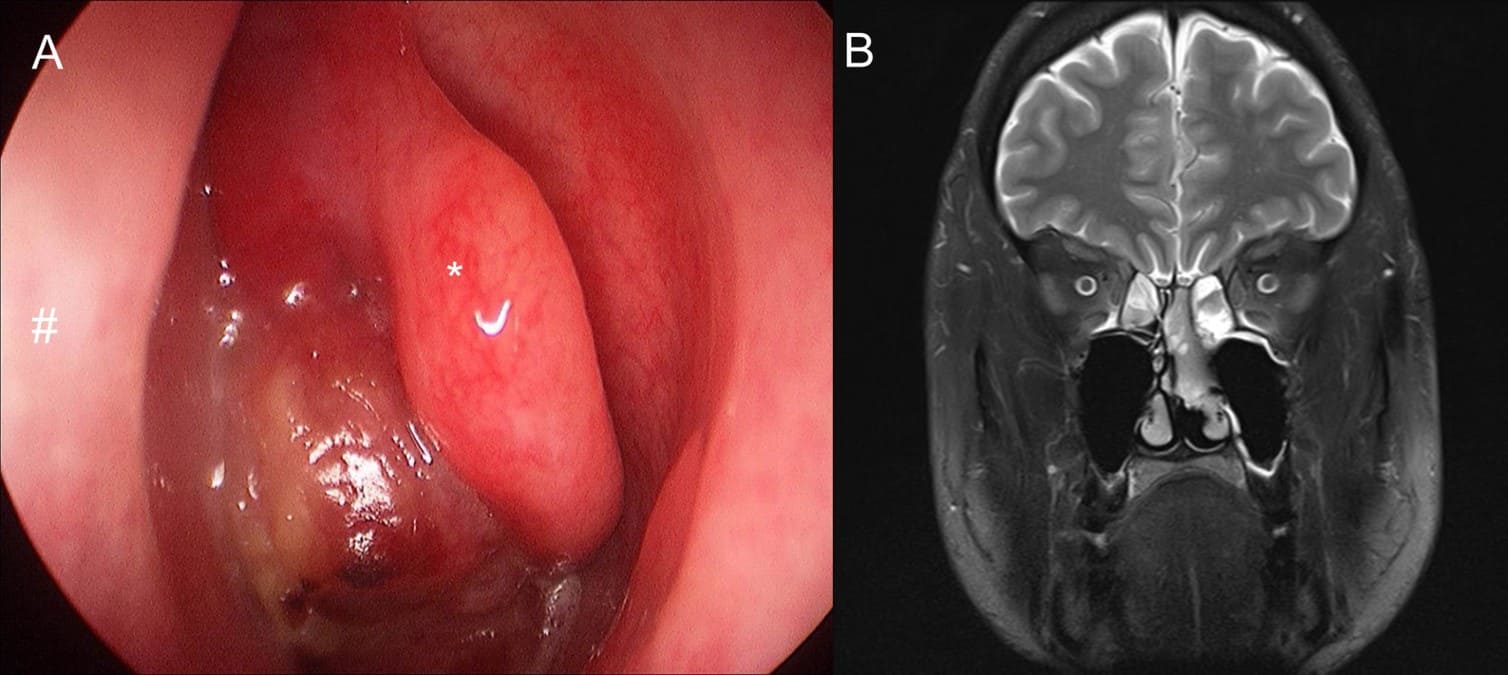
An example of an uncommon cause for smell loss – a nasal tumour

A more common cause of smell loss – inflammatory nasal polyps
Then we perform an objective assessment of smell in patients who feel they can’t smell. This is highly validated and objectifies the ability to identify, discriminate and determine a threshold for odorants.
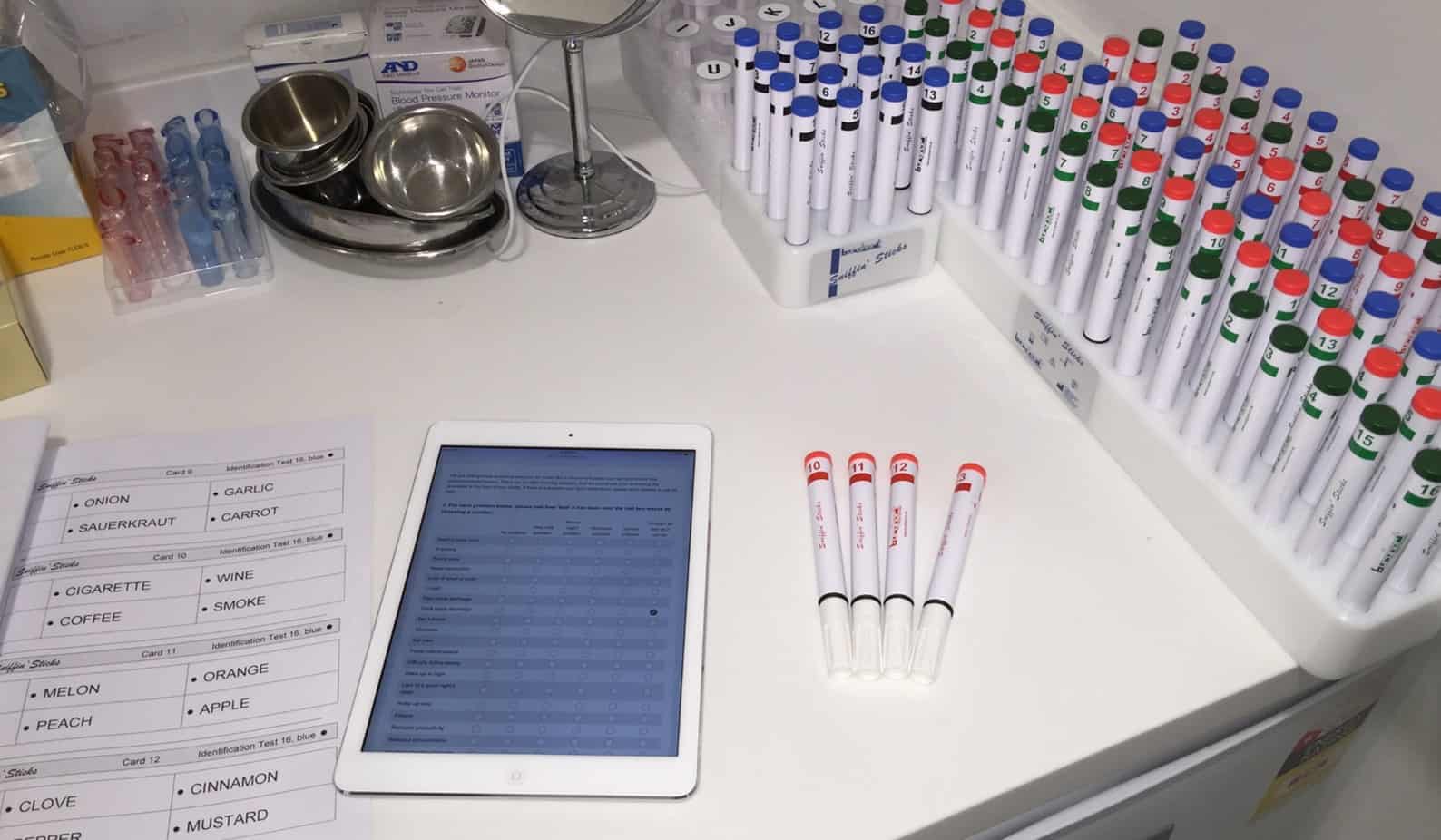
The comprehensive identification, discrimination and threshold testing we perform with Prof Harvey
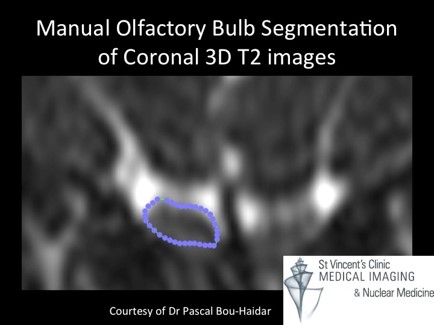
Finally, imaging is performed. This will often involve an MRI of the brain and the nerve of smell (the olfactory bulb and tract). The olfactory bulb can be measured and its volume is good reference as to whether an injury has occurred to this part of the smell system. Normal values are those above the 10th centile ( <45yro 58mm3, >45yro 46mm3). A neuroquant study is incorporated into this to assess the higher cognitive function.
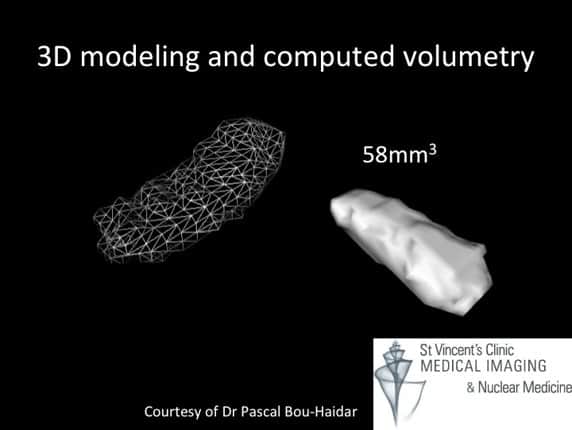
Measuring the olfactory bulb volumes has important diagnostic and prognostic implications
Measuring the olfactory bulb volumes has important diagnostic and prognostic implications
When we can’t smell it greatly affects daily function:
- Food intake
- Decrease appetite
- Around lower enjoyment
- Isolated from social experience
- Increase appetite
- Attempting to taste food
- Disruption of appetite suppression
- Decrease appetite
- Safety
- identifying spoilt food
- Fire, gas and smoke detection
- Anxiety
- In ability to perceive body odor
- Over use of perfume
- Impairs sex life
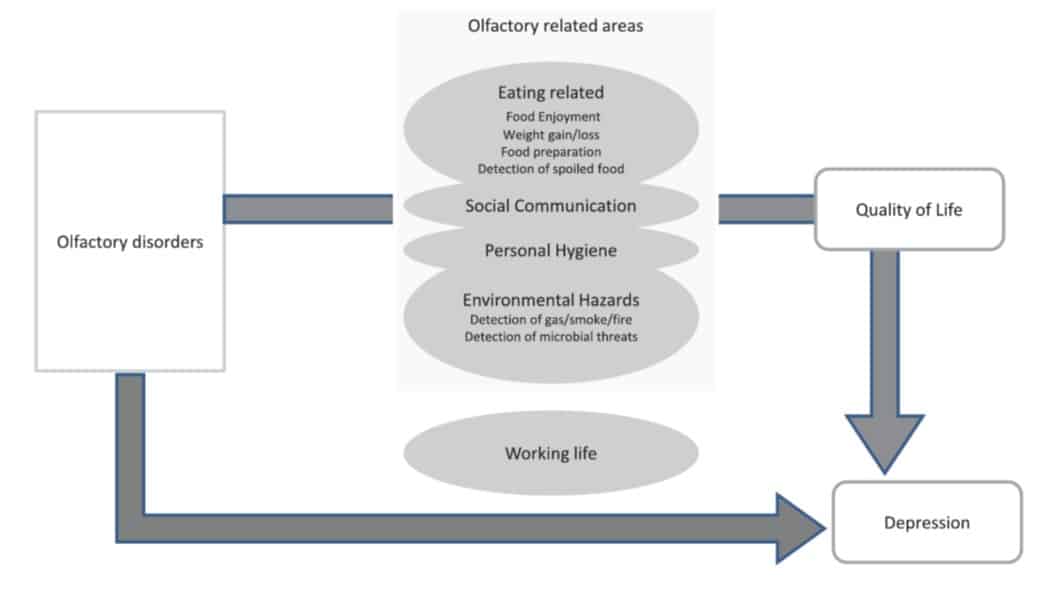
Adapted from: Croy I, Negoias S, Novakova L, Landis BN, Hummel T. Learning about the functions of the olfactory system from people without a sense of smell. PLoS ONE. 2012;7(3):e33365.
When these occur, it impacts our social life, communications with others, quality of life and may contribute to depression. This is especially true when smell loss becomes the ‘second’ sensory loss in an adult who might have lost sight or hearing.
What does it mean if we can’t smell and yet there is nothing wrong with the nose, sinuses or the nerve of smell itself?
I recent study in PLOS One has demonstrated that such, otherwise unexplained smell loss, is potential sign that our body’s biological clock is running out of time. The Olfactory system is one of the few partf of the central nervous system that can regenerate. It has been postulated that in adults 57-85yro, that when smell loss occurs and all other factors have been adjusted for (ie associated conditions that might also decrease life and potentially impact smell) that the mortality rate of those with anosmia is more than 3 time s(300%+) or an OR, 3.37 [95%CI 2.04, 5.57] that of those people that still had an intact smell sense.

Adapted from: Pinto JM, Wroblewski KE, Kern DW, Schumm LP, McClintock MK. Olfactory dysfunction predicts 5-year mortality in older adults. PLoS ONE. 2014;9(10)
And unfortunately, if that’s not depressing enough, there is a clear relationship with the loss of smell as preceding symptom of degenerative brain disease such as Parkinson’s disease and Alzheimers dementia:
| Condition | Age (95% CI) of disease | % with premorbid anosmia/hyposmia | Years preceding event |
| Parkinson’s | |||
| Ponsen et al, 2004 | 59.2+/-5.8 | 10% | 9 to 19 months |
| Alzheimer’s | |||
| Devanand et al, 2010 | 81.25+/-5.64 | 24% | 2-4 YRS |
But fortunately, there are many simple and local causes of smell loss. When we can’t smell, there is most likely to be post viral or sino-nasal cause, in which treatments are available. Even for those patients with olfactory centres that have been severely affected by viral events or external volatile injury, techniques such as olfactory re-training can greatly assist.
More about sino-nasal disorders and care: