
Adequate hearing is essential to maintain a connection with the outside world. In general terms there are 2 main components to our hearing, the conductive component and the sensorineural (nerve) component.
Both of these components can be affected by inherited and acquired conditions. This can range from simple mechanical problems such as wax impaction in the ear canal and fluid behind the ear drum, to molecular changes affecting cochlear hair cells and tumours compressing the nerve of hearing.
Any degree of hearing loss requires careful measurement and assesement. As there is a wide range of possible pathologies there is a wide range of treatments that may be required.
Acquired sensorineural hearing loss in adults, most likely reflects a varying balance of environmental-genetic interactions, the most frequent of which are age-related and noise-induced hearing loss. At this stage only a few genes have been associated with these traits. A good overview is found in ”Current concepts in age-related hearing loss: Epidemiology and mechanistic pathways” Yamasoba et al 2013. There are a number of other delayed onset genetic causes of hearing loss that present in adulthood that can be progressive, most of which are inherited in a autosomal recessive fashion. An important interaction pertinent to medical care is the observation that aminoglycoside-induced hearing loss is more likely in persons with specific variants in the mitochondrial genome (mtDNA).
Sensorineural hearing loss can also result from chronic suppurative ear disease, viral reactivation (see sudden sensorineural hearing loss syndrome), trauma, surgery, tumours (see vestibular schwannoma), Meniere’s Disease, cerebrovascular disease (strokes), ototoxic medications and other conditions such as otosclerosis that predominantly cause conductive hearing loss.

A moderate to large vestibular schwannoma (acoustic neuroma) causing a severe hearing loss. Due to it’s size it is causing a moderate degree of brainstem compression and requires microsurgical removal
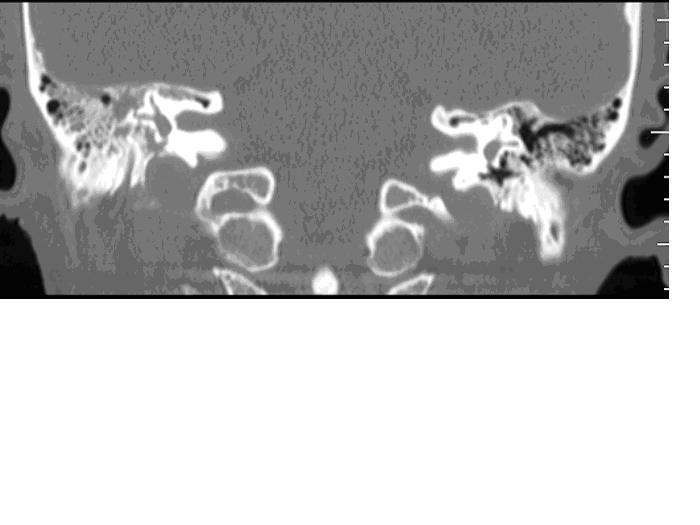
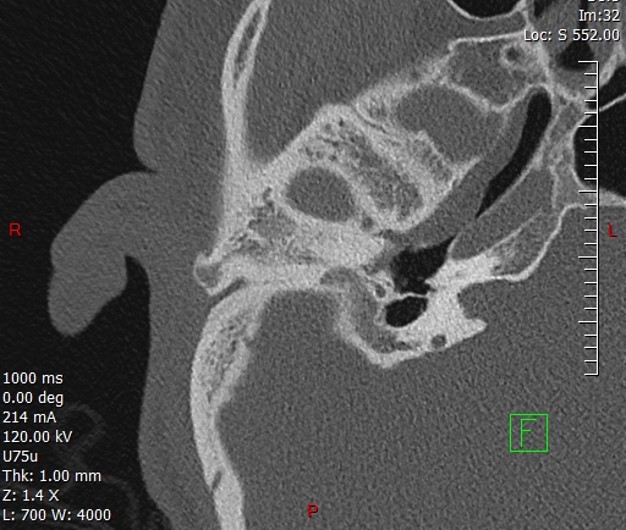
CT scan showing a fracture through the otic capsule (inner ear structures) causing complete hearing and balance loss on the right side
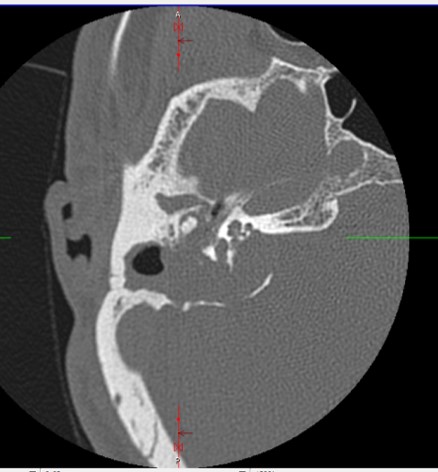
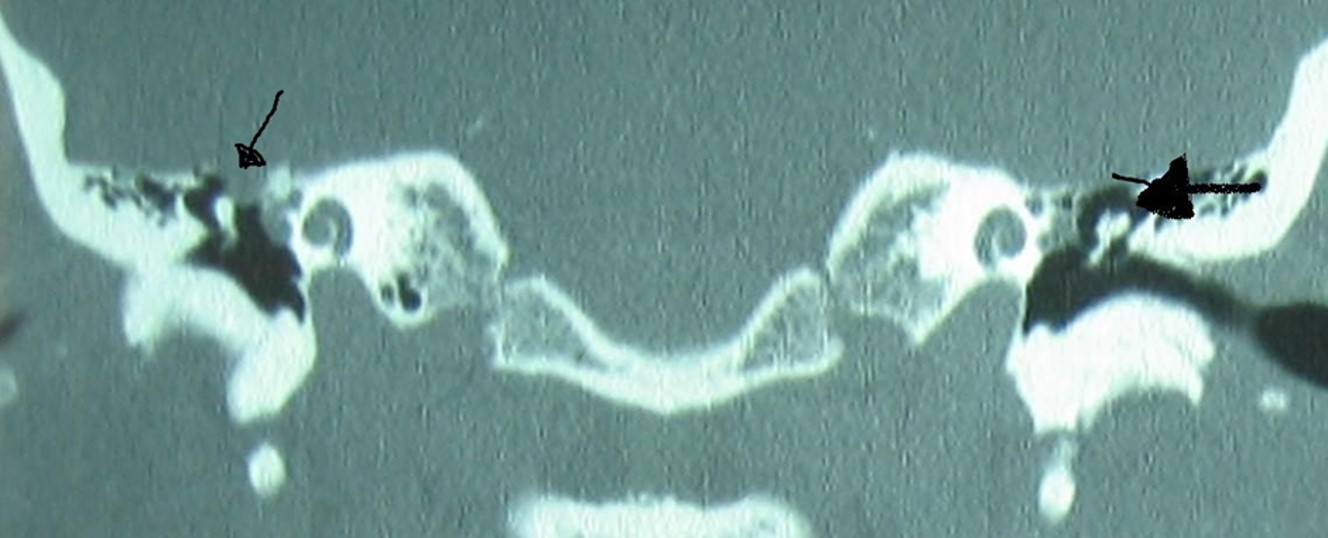
Petrous temporal bone cholesteatoma: extensive destruction of the inner ear causing complete sensorineural hearing loss, vestibular dysfunction and partial facial nerve paralysis
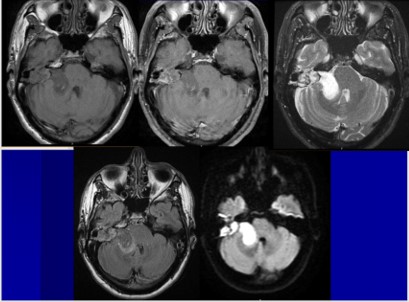
Series of MRI scans of the above case of petrous temporal bone cholesteatoma, with significant intracranial extension. The diffusion restriction confirms the diagnosis of a cholesteatoma
Genetic hearing loss can affect all categories of hearing loss, including the following: congenital, progressive, and adult onset; conductive, sensory, and neural; syndromic and nonsyndromic; high-frequency, low-frequency, or mixed frequency; and mild or profound. Genetic hearing loss may show patterns of recessive, dominant, or sex-linked inheritance and may be a result in mutation of both cellular or mitochondrial DNA. For an overview of hearing loss in childhood please click following link. Congenital hearing loss (permanent childhood hearing loss). Genetic testing currently is limited to a relatively small number of genes, but this is a rapidly expanding area, not only for children but for adults. Whilst currently it does not offer a treatment option it may provide information important for family planning and prognosis. For adults the clinical genomics unit at St Vincent’s Hospital provides an excellent service providing genetic counselling and testing. For appropriate patients a referral is often made. This also allows an expanding database of genetic information that can be accessed when further genes are identified in the future and ultimately a direct treatment option.
Summary of common causes of sensorineural hearing loss
Presbycusis (age related hearing loss) is the most common form of hearing loss. It is the predominant neurodegenerative disease of ageing. It is generally slowly progressive, symmetric and irreversible, and in some has a genetic predisposition. It classically affects the higher frequencies and in early cases causes hearing difficulties especially in the presence of background noise. It is estimated that 35-55% of age related hearing loss has a genetic component.
Noise induced hearing loss is the commonest preventable form of sensorineural hearing loss. Prolonged exposure to noise creates damage to cochlear hair cells, microscopic components of the inner ear that are responsible for converting sound waves into an electric neural signal that is perceived as sound. When exposed to loud noise the ear can react by creating a sensation of tinnitus or ringing in the ear. Initially this is self resolving and is termed a temporary threshold shift. Repeated and extended exposure to loud noise can then lead to permanent damage. As a general guidline permanent damage can occur after exposure to noise at 85dB after 8 hours. For every 3dB rise in noise input, the ear can last half that time. So at 88dB, 4 hours is the maximum exposure. 91dB 2 hours, 94dB 1 hour, 97dB 30 minutes, 100dB 15minutes and so on. As a guide to the level of environmental noise, a chainsaw runs at 100dB. The level of noise within a nightclub however also runs around the 100dB level.
Management of these and many other causes of sensorineural hearing loss involves minimising further damage, improving the quality of sound and the sound environment, and then consideration of hearing aids and other assistive listening devices. When maximal aiding and support are achieved and there remains significant hearing difficulties, cochlear implantation becomes an important part of overall hearing rehabilitation.
Causes of Conductive Hearing Loss
Wax
Complete occlusion of the external auditory canal (ear canal) with wax (cerumen)
Congenital atresia of the ear canal
CT scan demonstrating the abscence of an external auditory canal. Almost always in these cases the inner ear (or nerve function) is working normally, meaning that an implantable hearing aid of some form is likely to give a very good hearing result
Bony (exostoses) and soft tissue occlusion (medial canal stenosis) of the ear canal
Significant narrowing of the ear canal due to exostoses (bony growths resulting from exposure to cold water) Any small amount of water or wax is likely to completely block the canal and thus hearing plus or minus causing an infection

Medial canal stenosis: complete occlusion of the ear canal related to formation of chronic scar tissue secondary to recurrent infection and often an underlying dermatologic condition

Lateral canal stenosis; a situation where the pinna (external ear) slides forward and predisposes to skin and wax blockage as well as creating problems fitting hearing aids. More common in the older ear.
Tympanic membrane perforation

Medium to large perforation of the right tympanic membrane (ear drum). This results in a moderate hearing loss and susceptibility to infections
Middle ear effusion

Right middle ear effusion (fluid behind the ear drum). The appearance is of a mildly inflamed drum with thick fluid trapped, often referred to as glue ear: common in children, and in general terms if present for more than 3 months is likely to require insertion of ventilation tubes or grommets.

Watery fluid trapped behind the ear drum. Note the appearance of air bubbles. This is common after a cold and is likely to clear in days to weeks
Ossicular chain abnormalities; Otosclerosis, Lateral chain fixation, ossicular erosion, ossicular dislocation

Surgical treatment of otosclerosis. Bypass of a fixed stapes bone with a small piston (4.5mm long and 0.4mm diameter) through a surgically created hole through the footplate of the stapes bone
Meningoencephalocele: a CT scan illustrating brain extending into the ear and resting on the malleus, creating a conductive hearing loss
Meningoencephalocele: a condition where the tegmen (roof of the ear, floor of the brain) becomes dehiscent, and extends into the ear This can cause hearing loss and creates a risk of meningitis.
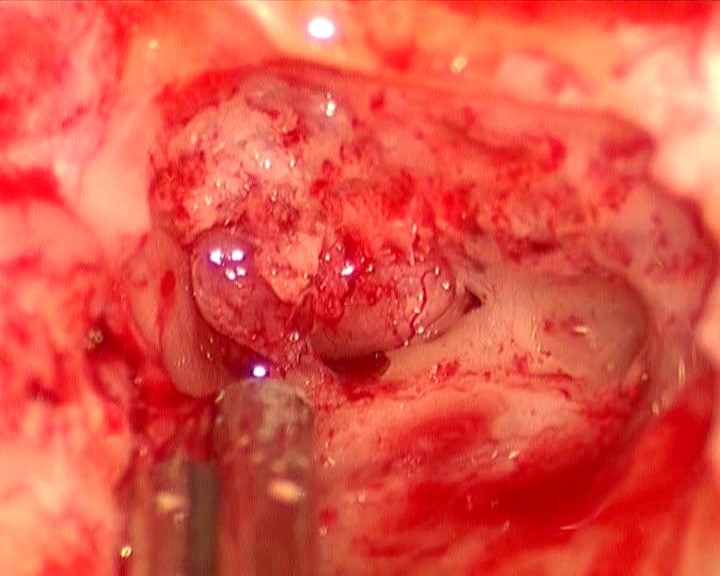
This is an intraoperative picture during a repair of the tegmen
Chronic suppurative ear disease, severe retraction and cholesteatoma

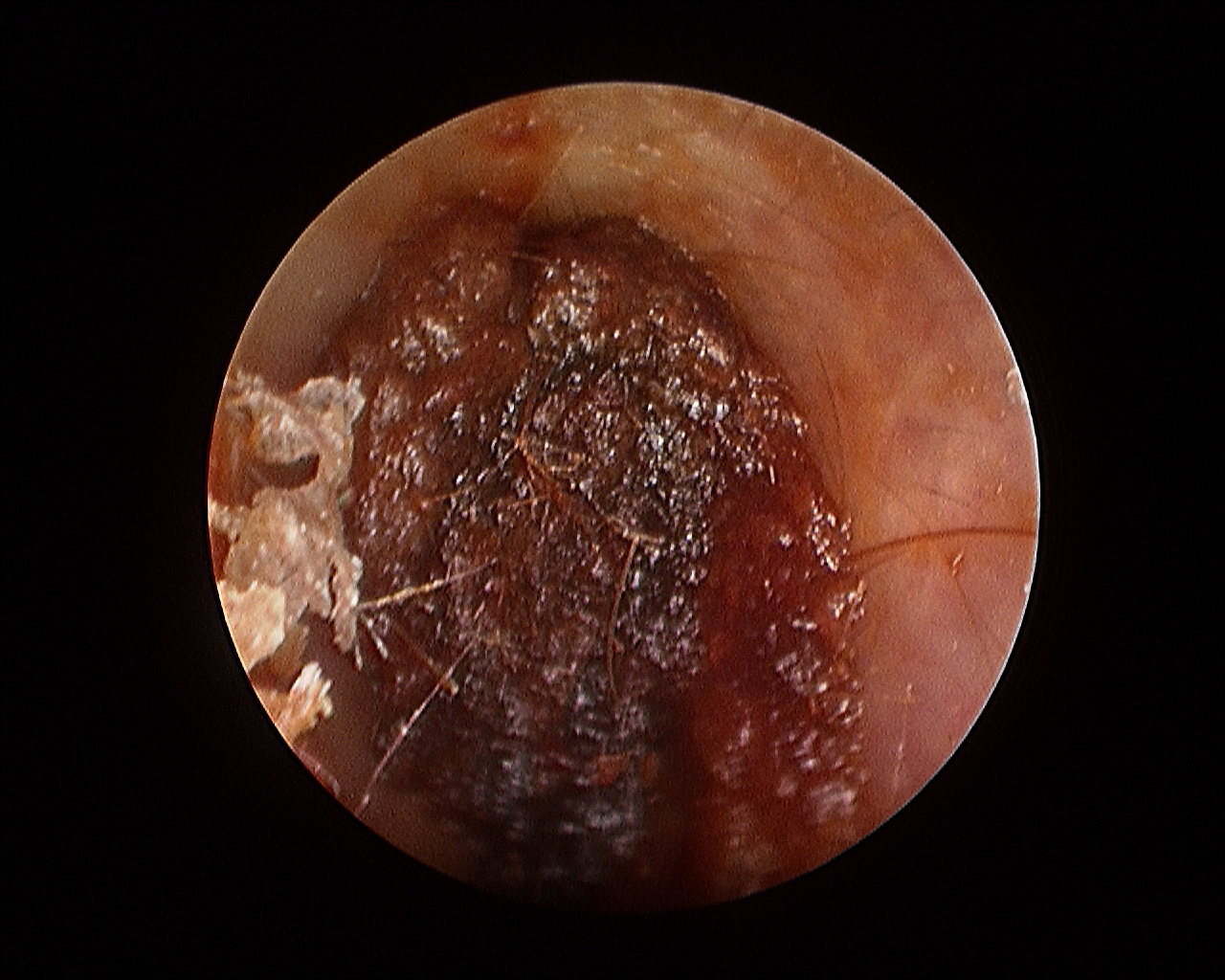
Severe retraction of the ear drum with evidence of an effusion. This is the result of longstanding eustachian tube dysfunction
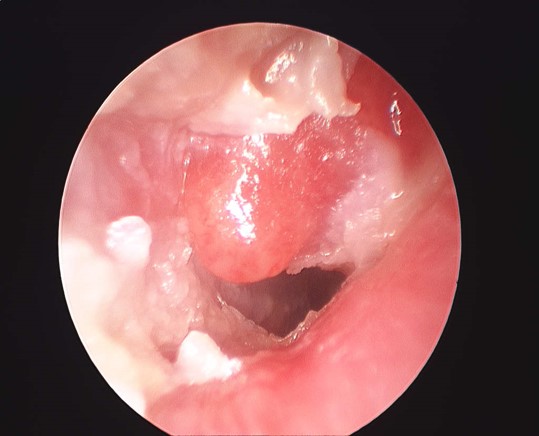
Cholesteatoma. An locally destructive process that can erode the bones of hearing, invade the inner ear, affect the facial nerve and extend into the brain. In this picture a ‘sentinel’polyp is seen

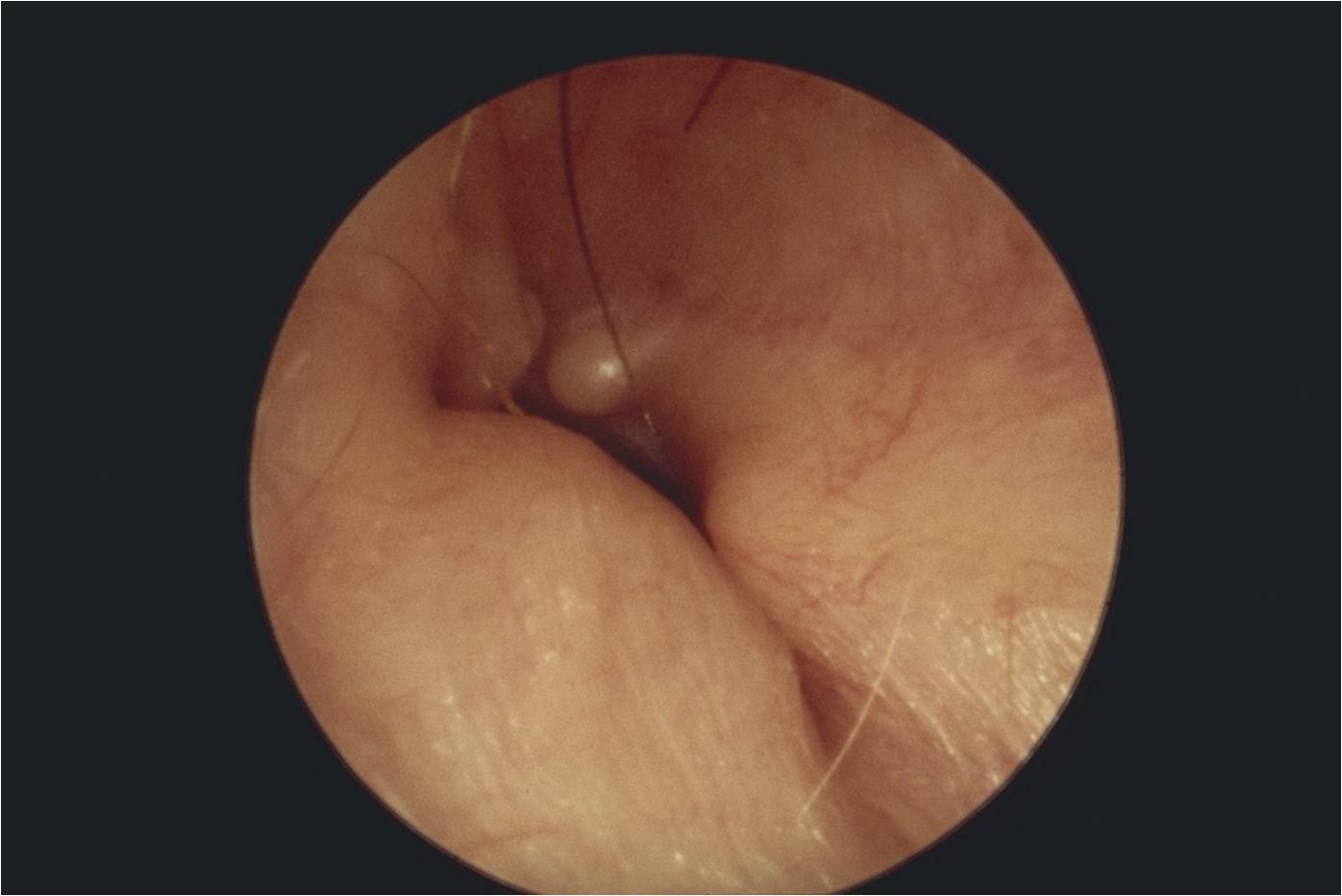
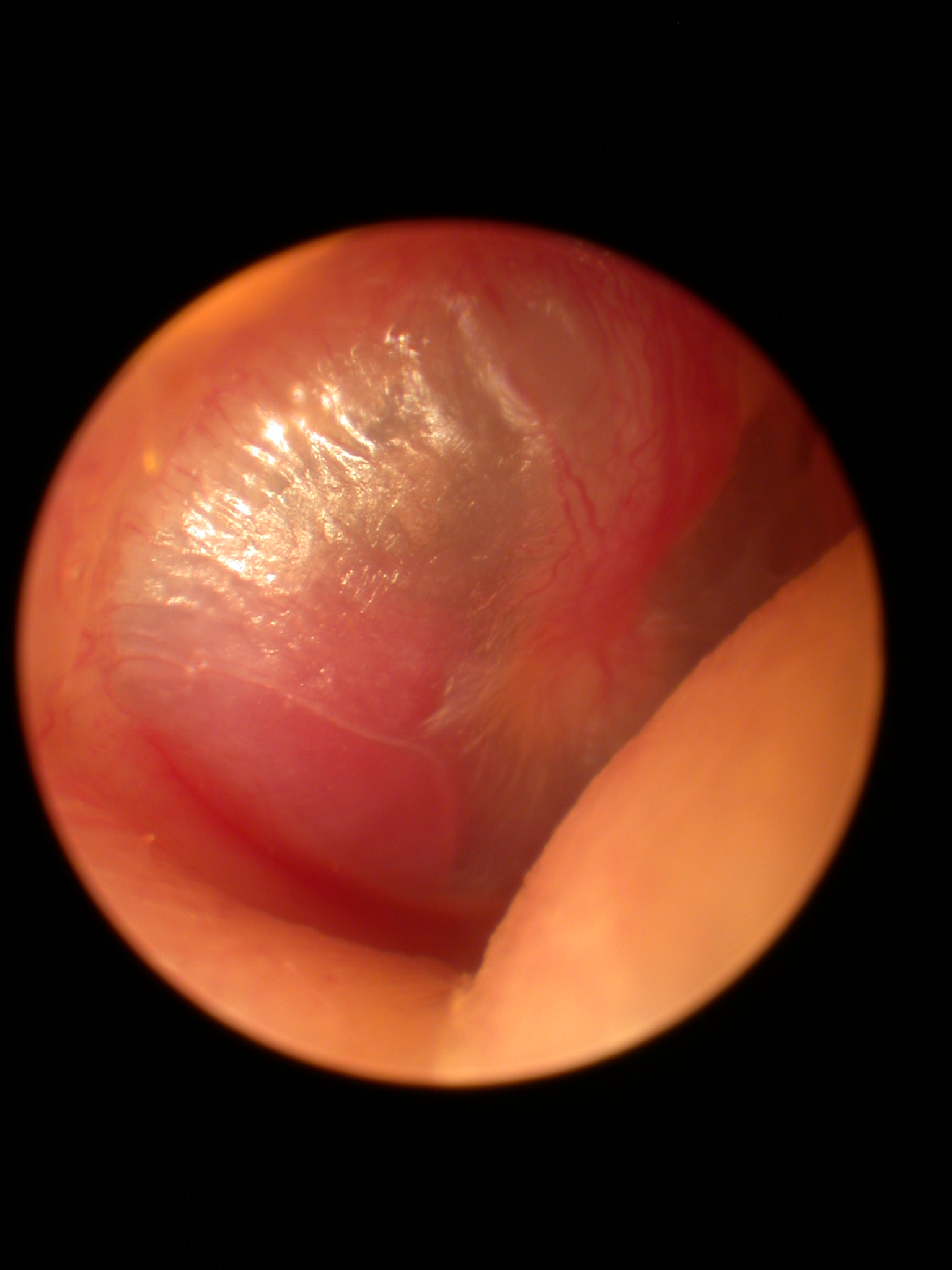
Congenital cholesteatoma; one of the causes of á white mass behind the ear drum’. Essentially a skin cyst present at birth that can expand and cause local destruction.
Paragangliomas (glomus tumours)
Glomus tympanicum, or more accurately a paraganglioma confined to the middle ear.
Malignant tumours: Squamous cell carcinoma (SCC) of the temporal bone.
Predominantly arising initially from skin.